
Submitted by Seemaab Ali, MD, PhD, and Scott Kulich, MD, PhD.
Clinical History
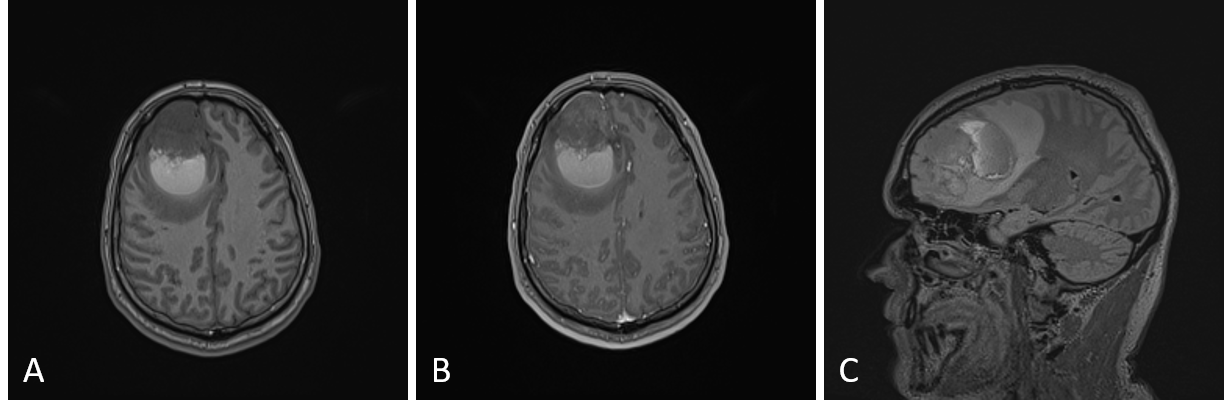
The patient is a male in his 30s who presented with weeks of progressive headaches with nausea and vomiting. MRI of the brain identified a right frontal cystic mass lesion with patchy, heterogenous contrast enhancement, calcifications, blood products, and surrounding vasogenic edema (Figure 1).
Cytologic and Histologic Findings
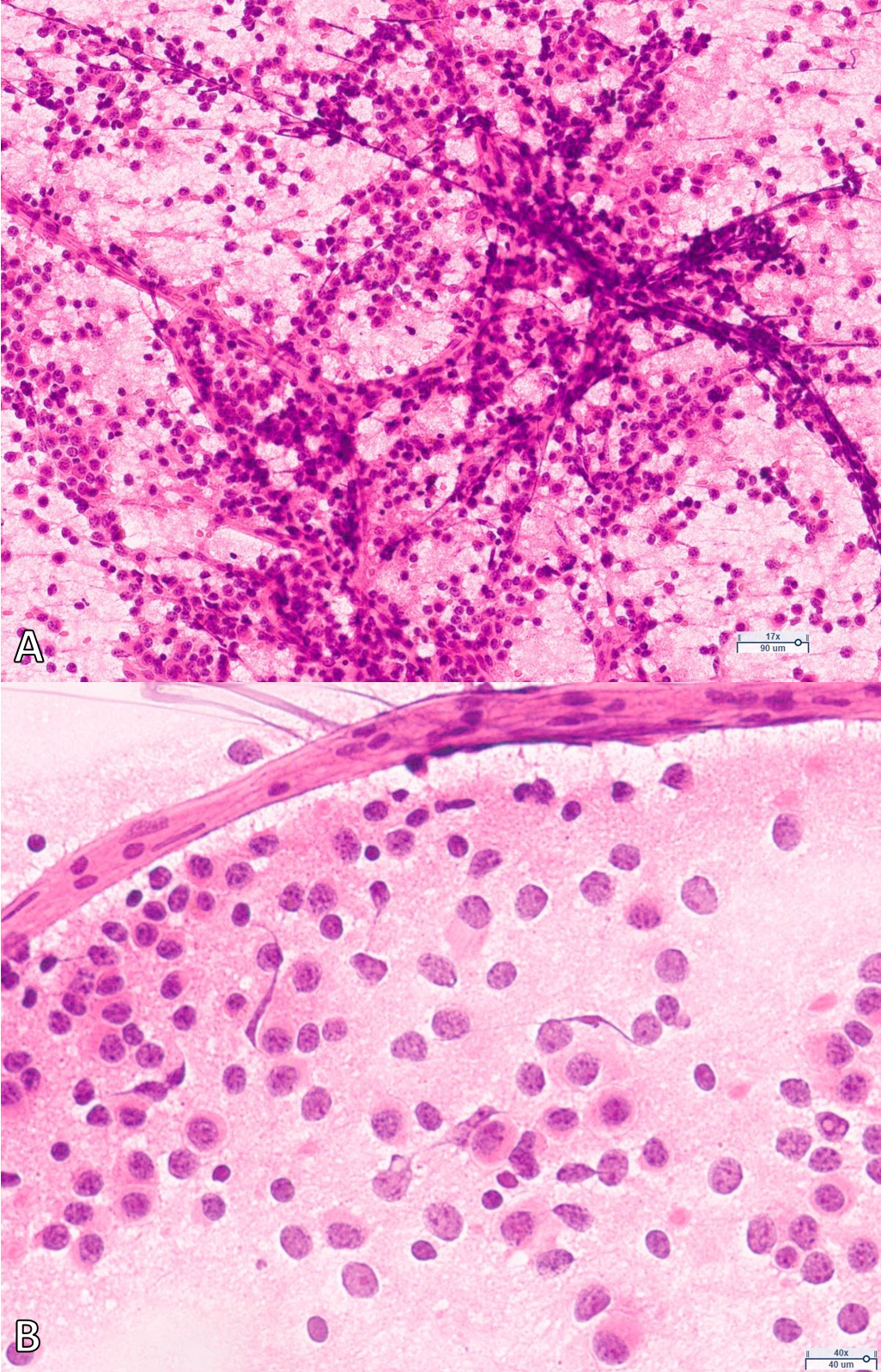
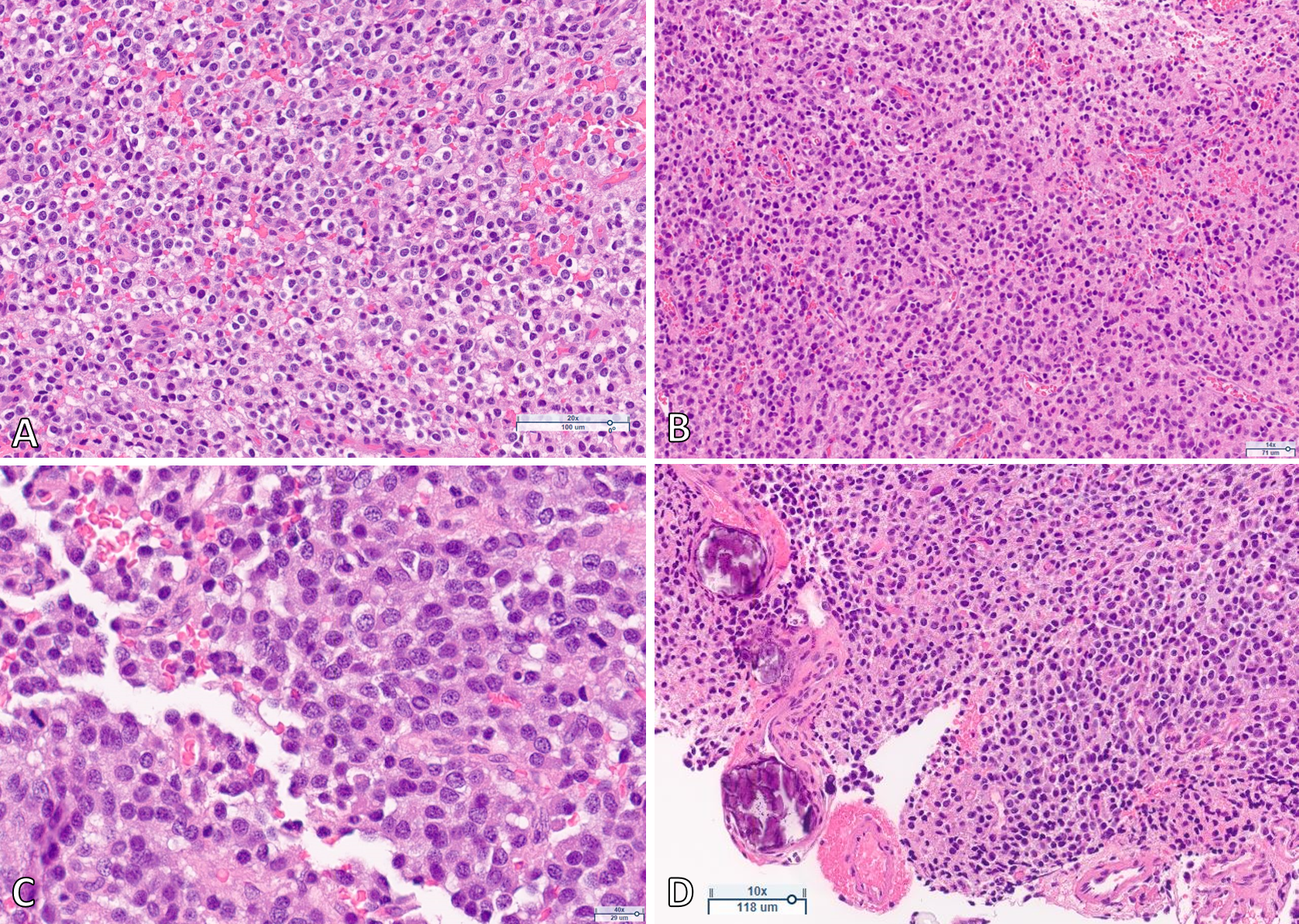
Intraoperative cytology preparations show a cellular glial neoplasm with round to ovoid nuclei and scant cytoplasm associated with a fine vascular network (Figure 2). Histologic sections demonstrate an infiltrative neoplasm composed of neoplastic cells with small, round nuclei with either cytoplasmic clearing or scant eosinophilic cytoplasm (Figure 3A). Scattered calcifications are present (Figure 3D). Mitoses are frequent, focally exceeding 10 per 10 high power fields (Figure 3C). Endothelial proliferation is not appreciated, despite a dense network of branching capillaries (Figure 3B). Necrosis is not present.
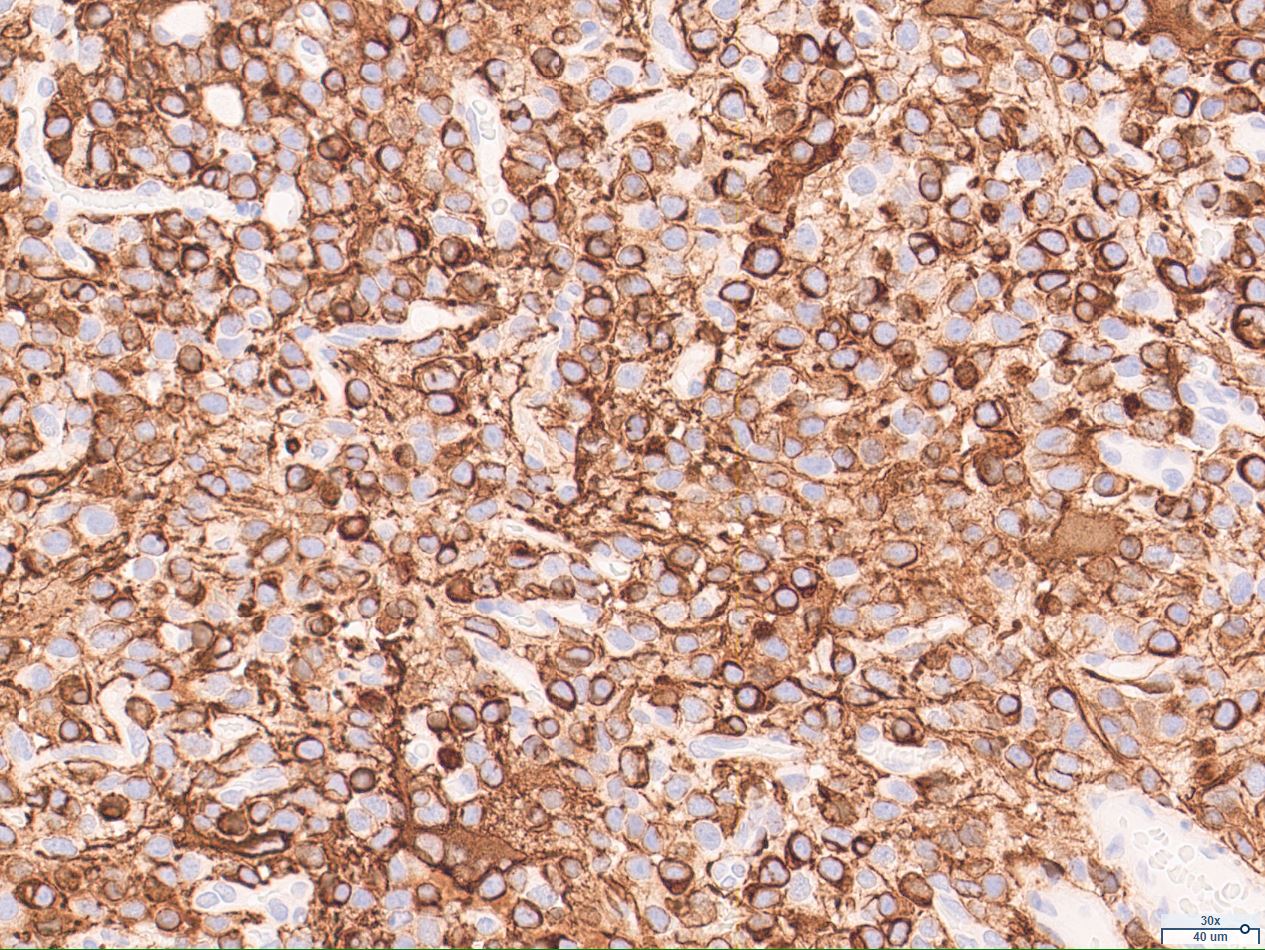
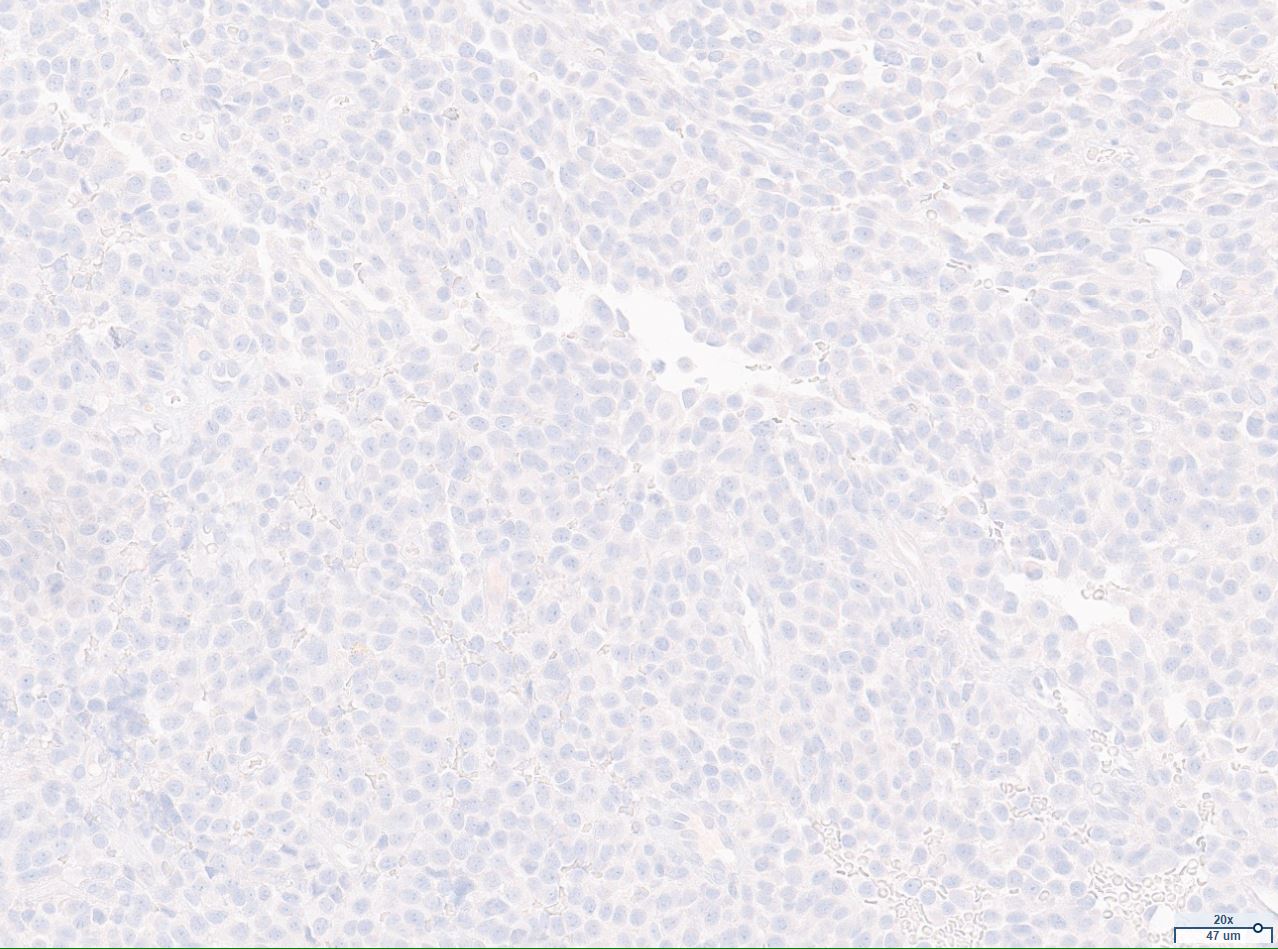
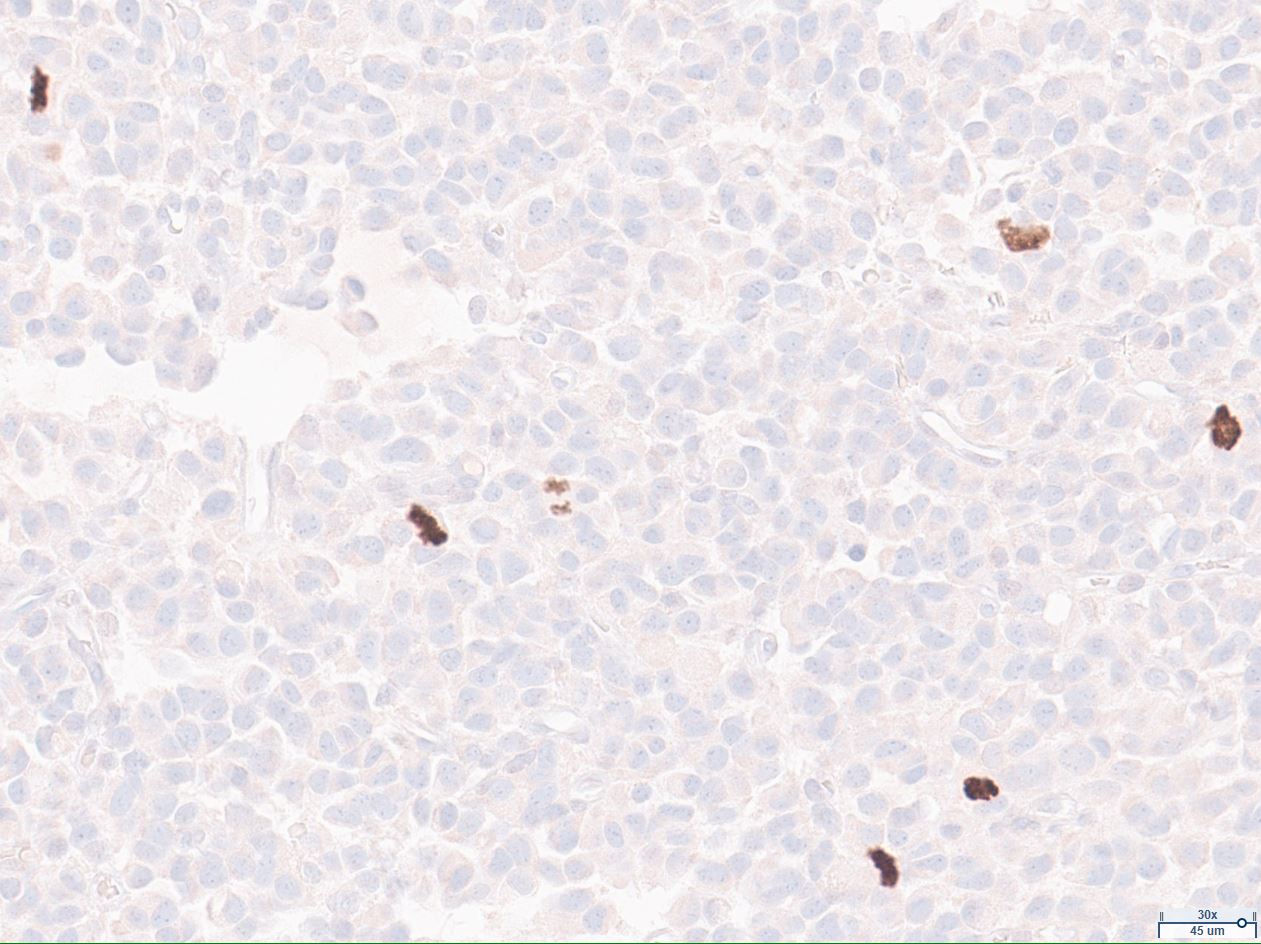
Immunohistochemical stains for GFAP and Olig2 highlight the glial nature of the tumor. GFAP demonstrates a thin perinuclear rim of positive staining around tumor cells (Figure 4). Staining for the IDH1 R132H mutation is negative (Figure 5). ATRX is retained and p53 is non-clonal. EGFR shows only weak to moderate intensity staining. NeuN and CD34 are negative in neoplastic cells. The Ki-67 proliferative index of the tumor is up to 15%. PHH3 highlights significant mitotic activity (Figure 6).
Although the diagnosis of a specific WHO entity was favored, an initial morphologic diagnosis of “diffuse infiltrating glioma, mitotically active” was rendered. Molecular studies were requested to confirm this morphologic impression.
Diagnosis and Discussion